Editor’s Note
This article is intended for educational purposes for ophthalmologists, optometrists, glaucoma specialists, ophthalmic technicians, and healthcare providers interested in tonometry, glaucoma screening, and corneal-independent approaches to intraocular pressure assessment. Technique guidance in this article reflects direct training experience across thousands of clinical users by the Diaton training team.
For decades, Goldmann applanation tonometry (GAT) has served as the clinical reference standard in eye care, and its role in glaucoma management remains well established. But GAT — like all corneal tonometry — rests on one key assumption: that the cornea being measured behaves in a predictable biomechanical way.
That assumption is increasingly tested in modern practice.
Millions of patients have undergone refractive procedures such as LASIK, PRK, or SMILE. Millions more present with naturally thin corneas, altered corneal hysteresis, age-related structural change, keratoconus, scarring, edema, or other conditions that can make corneal-based intraocular pressure (IOP) readings harder to interpret — because the surface being measured has itself changed.
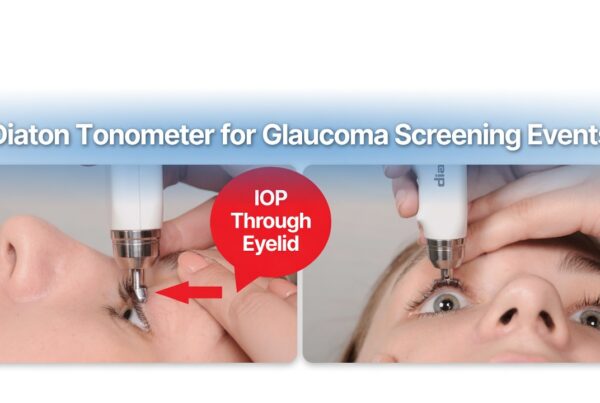
The Diaton® transpalpebral tonometer offers a different approach. Instead of measuring through the cornea, it takes its reading through the upper eyelid, over the sclera, bypassing corneal variables entirely. This article explains the clinical rationale behind corneal-independent IOP screening, the mechanical principle behind the Diaton system, and why it can serve as a consistent, repeatable, and technician-friendly screening tool in everyday clinical use.
1. Why Modern Eye Care Needs a Corneal-Independent Perspective
Traditional corneal tonometers estimate IOP by measuring the force required to flatten a defined area of the cornea. The result is inherently shaped by the physical properties of the cornea itself, including:
- central corneal thickness (CCT)
- corneal rigidity
- corneal hysteresis
- post-surgical structural change
- scarring or irregularity
In structurally typical corneas, that dependency may be clinically acceptable and familiar. But in post-refractive or otherwise altered corneas, it becomes more relevant.
Post-LASIK and Post-Refractive Patients
LASIK, PRK, and SMILE permanently alter corneal thickness and structural elasticity. In these eyes, corneal applanation readings may be influenced by the biomechanical changes introduced by surgery. This is one reason clinicians often interpret post-refractive IOP values with added caution.
Biomechanical Variables Beyond Pachymetry
Even when central corneal thickness is known, pachymetry alone does not fully resolve the issue. A numeric CCT value cannot fully account for:
- individual corneal hysteresis
- focal or irregular scarring
- ectatic change
- altered elasticity from surgery or aging
- edema or surface pathology
Where Diaton Extends the Clinical Toolkit
Because the Diaton tonometer measures through the upper eyelid over the sclera, those corneal variables do not enter the measurement pathway. This does not replace the historical role of corneal tonometry. Rather, it adds a complementary, corneal-independent screening option for the growing population of patients whose corneal-based readings may be more difficult to interpret.
2. The Measurement Principle: Fixed Mechanics, Not Corneal Deformation
The Diaton is built around a ballistic transpalpebral measurement principle grounded in Newton’s second law of motion:
F = ma
A small internal rod (the floater) performs a short, controlled free-fall inside the device, contacts the eyelid tissue overlying the sclera, and rebounds. The device evaluates the deceleration and rebound characteristics of that interaction — not corneal flattening.
Three parameters are fixed by design and manufacturing calibration:
1. Fixed Internal Mass
The floater is manufactured to a precise mass specification.
2. Fixed Fall Distance
The drop height is mechanically fixed during production and calibration.
3. Gravity-Driven Movement
The fall follows a controlled gravitational path, provided the device is held vertically.
Because these inputs are fixed by design, the Diaton’s internal measurement engine is mechanically consistent and does not depend on corneal deformation. In practical terms, this means that variation between readings is more likely to reflect positioning, tissue contact, or patient factors than variability in the device’s underlying measurement principle.
That distinction is central to understanding why Diaton can function as a corneal-independent screening tool.
3. Where Diaton Can Be Especially Useful
Corneal-independent IOP screening is particularly relevant for:
- post-LASIK, post-PRK, and post-SMILE patients
- thin corneas or atypical corneal biomechanics
- keratoconus or irregular corneal surfaces
- corneal scarring or edema
- patients wearing scleral or therapeutic contact lenses
- post-corneal-surgery patients
- patients who are highly sensitive to corneal contact
- screening environments where speed, comfort, and portability matter
These use cases matter not only in ophthalmology and optometry clinics, but also in:
- emergency departments
- urgent care settings
- hospital-based screening programs
- mobile outreach initiatives
- broader healthcare environments where portable IOP screening may be valuable
4. Why Technique Matters in a Gravity-Driven System
The reason Diaton can produce consistent, repeatable readings comes down to the fact that its internal physics are fixed. The floater’s mass, drop height, and gravity-driven motion do not change from patient to patient.
The key variable is therefore where and how the floater makes contact. That is a function of positioning and technique — and, importantly, it is a straightforward and trainable technique, not an arbitrary one.
For most users, once trained, proper placement becomes routine. Understanding the mechanics behind the technique is still valuable because it explains why the device is consistent when used correctly, and how to recognize the few factors that can influence a reading.
5. Three Core Technique Principles for Consistent Readings
 a) a) |  |
A. Device Verticality
The Diaton emits a continuous beep until it reaches true 90° vertical alignment. Once correct verticality is achieved, the beep stops.
If a reading is taken while the device is still tilted, the display shows the letter “L”, indicating that the free-fall path was angled and the measurement should be repeated.
Verticality matters because the Diaton’s measurement principle depends on a straight, unobstructed free-fall of the internal floater.
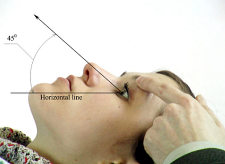
B. Horizontal Head Positioning
This is one of the most important ways Diaton technique differs from traditional corneal tonometry.
With Goldmann, Tonopen, or iCare, the patient’s head is typically upright, because those devices do not depend on gravity acting through the eye in a specific direction. Diaton is different. Because its measurement depends on a gravity-driven free-fall, the patient’s head needs to be as horizontal as possible so the drop occurs at the correct angle relative to the eye.
This can be achieved either:
- with the patient supine, or
- with the patient seated and reclined, with the chin gently guided upward until the head is as horizontal as is comfortable
From there, the patient extends a thumb at roughly a 45° angle and looks at it. This helps position the eye so the examiner can access the tarsal plate and sclera without pulling excessively on the eyelid.
If lifting the lid still creates noticeable tension, lowering the thumb slightly usually drops the gaze further and clears the cornea more naturally.
C. Correct Target Zone
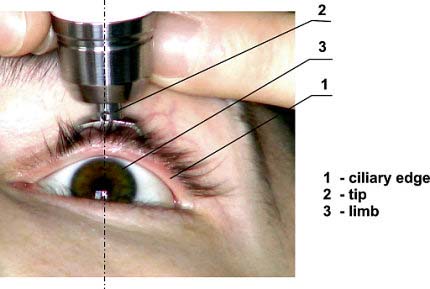
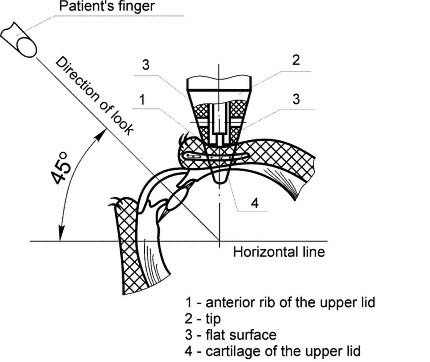
The upper eyelid should be lifted gently just enough to clear the cornea — think of it as clearing the edge of an imaginary contact lens covering the cornea.
The Diaton tip should land over the tarsal plate and sclera, approximately 1–2 mm above the limbus.
This target matters because the device is designed to measure through the eyelid over the sclera, not over the cornea.
6. Predictable Causes of Higher or Lower Readings
One of the strengths of the Diaton system is that when technique affects the reading, the direction of that effect is usually predictable rather than random.
If the lid is pulled too tightly
Extra tension in the upper lid tends to produce a reading that is higher than the true IOP because the tissue at the contact point becomes tighter.
If the floater contacts the cornea instead of the sclera
The reading tends to be lower, because the cornea is a softer tissue surface than the intended scleral target zone.
In both cases, the device is still evaluating the surface it contacts. The goal of technique is to ensure that the contact occurs at the correct anatomical target — the tarsal plate over the sclera — with minimal added lid tension.
This predictable relationship is helpful in training because it allows users to understand not only that technique matters, but how it matters.
7. Multi-Reading Confirmation, User Judgment, and Device Feedback
Like any precision tonometer, Diaton does not remove the need for clinical judgment. Instead, it gives the user real-time feedback to help confirm whether a reading is reliable.
A trained user typically takes 2–3 readings per eye, and occasionally more — up to 6 — if patient cooperation or tissue conditions are variable.
The device supports the user with several signals
- Verticality beep — confirms whether the device is properly aligned
- “L” indicator — flags an off-vertical reading
- Long beep — signals that consecutive readings are in agreement and the user has enough consistent data to accept the averaged result
If readings do not agree, the device does not signal completion, and the user should continue until a stable cluster is obtained.
This is not fundamentally different from other tonometers. Goldmann, Tonopen, and iCare also depend on examiner technique, positioning, and judgment regarding whether a reading is trustworthy. Diaton is the same in that respect: it is a precision clinical instrument that rewards attentive, trained use, while offering built-in signals to support that use.
8. Why Technique-Related Differences Should Be Understood, Not Feared
Where published comparisons show a directional gap between Diaton and corneal tonometry — especially in eyes without obvious corneal pathology — technique factors should be considered as one possible explanation.
Because Diaton depends on:
- gravity-aligned positioning
- horizontal head setup
- correct scleral targeting
- appropriate lid handling
differences in examiner training or technique standardization can influence results if these factors are not applied consistently.
That does not mean Diaton is unusually fragile or difficult. It means it has its own technique requirements, just as Goldmann has its own. Eye care professionals are already accustomed to the fact that tonometry is not purely “push button” medicine; correct positioning and examiner awareness matter with every device.
The Diaton equivalent of that attentiveness is:
- not over-tensioning the lid
- not allowing the lid to slide onto the cornea
- keeping the patient’s head horizontal
- confirming vertical alignment before accepting a reading
Once those principles are understood, the device becomes highly straightforward to use.
9. Training and Practice Before Patient Use
 a) a) |  b) b) |
New users can validate their own technique before ever touching a patient by using two simple training methods:
Calibration Test Eye
The carry case includes a fixed-reference test eye designed to help users practice toward the expected 20 mmHg reference reading. Practicing on this test eye helps confirm that positioning and activation technique are sound.
Practice on a Finger
Practicing on one’s own finger at a consistent position helps the user understand how little pressure is actually required — only a gentle activation of roughly 1 mm to release the floater.
With a brief introduction and supervised practice, most users learn the Diaton workflow quickly.
10. Designed for Busy Clinics and Ophthalmic Technicians
One of Diaton’s practical strengths is that it is not only a physician tool — it is also well suited to technician-driven workflows.
In many ophthalmology and optometry practices, ophthalmic technicians perform the initial workup and help keep clinic flow moving. A device that is cumbersome, intimidating, or difficult to learn may not be adopted efficiently, even if the underlying technology is compelling.
Diaton helps address that challenge through:
- portable handheld design
- no corneal contact
- no anesthetic drops
- no disposable tips
- clear device feedback signals
- straightforward onboarding for technicians and staff
That combination makes it especially useful in busy clinics, where screening efficiency and ease of implementation matter just as much as the measurement principle itself.
11. Practical Advantages Beyond the Measurement Pathway
The value of Diaton is not limited to its transpalpebral mechanics. It also offers several practical workflow and ownership advantages:
Corneal-independent measurement
Useful in patients with altered corneal biomechanics, post-refractive eyes, and other situations where corneal-based readings may be more difficult to interpret.
No corneal contact
Improves comfort and avoids direct contact with the corneal surface.
No anesthetic drops
Removes an extra step from the screening workflow.
No disposable tips or covers
Helps reduce recurring supply costs and simplify logistics.
Portable, technician-friendly design
Useful in ophthalmology and optometry clinics, hospitals, emergency departments, and outreach or mobile screening settings.
12. What Diaton Is — and Is Not
Diaton is best understood as a corneal-independent screening and assessment tool that complements traditional tonometry.
It is especially valuable when:
- corneal biomechanics may limit interpretation of corneal-based readings
- portability and comfort matter
- technician-friendly implementation is important
- a broader screening workflow is needed
It is not a claim that corneal tonometry has no role. Goldmann applanation remains a foundational method in glaucoma care. Rather, Diaton expands the clinician’s options by offering an additional IOP perspective that bypasses corneal variables entirely.
That is the right way to understand its role in modern eye care: not as a rejection of traditional tonometry, but as a strategic extension of it.
13. Diaton’s Role in the Evolving Tonometry Landscape
Goldmann applanation tonometry remains historically important and clinically familiar. But as the population of patients with surgically altered or biomechanically atypical corneas continues to grow, practices increasingly benefit from a complementary, corneal-independent screening tool — one that is mechanically consistent by design and practical for real-world clinic workflows.
The Diaton tonometer answers that need by offering:
- a through-the-eyelid, scleral measurement pathway
- a corneal-independent perspective on IOP
- a portable, patient-friendly workflow
- and a technician-friendly screening tool for busy clinical environments
Conclusion
The Diaton® transpalpebral tonometer expands modern eye care by bridging the gap between established tonometry traditions and changing patient realities.
It does not seek to replace the historical role of corneal tonometry. Instead, it provides a mechanically consistent, corneal-independent screening option that can complement existing practice — especially in patients with altered corneal biomechanics, post-refractive surgery histories, corneal pathology, or clinic workflows where portability and simplicity matter.
For ophthalmologists, optometrists, ophthalmic technicians, hospitals, and screening programs, Diaton offers something increasingly valuable in modern glaucoma care:
- a corneal-independent perspective on IOP
- a through-the-eyelid screening workflow
- a user-friendly tool that can be learned and implemented quickly
- and a practical way to expand glaucoma detection beyond the limitations of corneal measurement alone
In an era where glaucoma screening must adapt to more complex corneas and more demanding workflows, Diaton helps clinics see beyond the corneal blind spot.
Frequently Asked Questions
Why is Diaton considered a consistent, repeatable tonometer?
Its measurement mechanism is built on fixed physical constants — a fixed floater mass, a fixed drop height, and gravity as the driving force. Because these baseline inputs are fixed by design, the device’s internal measurement engine is mechanically consistent from reading to reading. In practice, any variation is more likely to reflect positioning, tissue contact, or patient factors than the device’s underlying measurement principle.
Does lid placement affect the reading?
Yes — and predictably so. Placement over the tarsal plate and sclera, the intended target, gives the standard clinically validated result. Extra lid tension tends to read slightly higher, while contact drifting onto the cornea tends to read lower, because the cornea is a softer surface. In every case, the device is measuring the surface it contacts; proper technique ensures that the correct anatomical target is being measured.
How does a user confirm that a Diaton reading is reliable?
The user typically takes 2–3 readings per eye, guided by the device’s feedback signals:
- the verticality beep
- the “L” alignment flag
- and the long beep when consecutive readings agree
The user also watches for blink, lid slippage, squeezing, or movement during the measurement. If readings do not agree, additional readings should be taken until a stable cluster is reached.
How can a new user verify they are using the device correctly?
By practicing on the fixed-reference calibration test eye included with the device, which is designed to help users practice toward the expected 20 mmHg reference reading, and by practicing on their own finger to understand the minimal activation pressure required.
Can Diaton be used by ophthalmic technicians?
Yes. With brief training and supervised practice, ophthalmic technicians can learn Diaton’s positioning and measurement workflow quickly. The device’s verticality beep, tilt indicator, and multi-reading confirmation help support consistent use in busy clinic environments.
Why might a Diaton reading differ from Goldmann in a post-LASIK eye?
Because the two devices measure through different tissue pathways. Goldmann depends on corneal biomechanics, while Diaton bypasses the cornea and measures through the eyelid over the sclera. In eyes with altered corneal structure, those different pathways may produce different values, which is why Diaton can provide a useful corneal-independent screening perspective.
Learn more about Diaton Tonometer:
- Diaton product page
- 100 Questions and Answers on Diaton
- How to use the Diaton Tonometer technique
- Diaton in post-LASIK / corneal pathology
- Diaton in emergency medicine / broader screening environments
- Glaucoma screening / glaucoma awareness
Learn more about Diaton Tonometer: www.TonometerDiaton.com
Contact Team Diaton via Phone: 1-877-342-8667
Editor’s Note:
This article is intended for educational purposes for eye care professionals and healthcare providers interested in tonometry, glaucoma screening, and corneal-independent approaches to intraocular pressure assessment.