Diaton Tonometer for Glaucoma Screening | Corneal-Independent IOP Measurement
Editor’s Note
This article is intended for educational purposes for ophthalmologists, optometrists, glaucoma specialists, ophthalmic technicians, and healthcare providers interested in tonometry, glaucoma screening, and corneal-independent approaches to intraocular pressure assessment. It is not intended to dismiss the role of Goldmann applanation tonometry, but to place corneal-dependent and corneal-independent IOP measurement in a more complete clinical context.
For decades, Goldmann applanation tonometry (GAT) has served as the most widely recognized clinical reference point in glaucoma care. It remains deeply important in eye care practice. Yet Goldmann, like most other commonly used tonometers, shares a basic dependency: it measures through the cornea.
That dependency matters.
In patients with relatively normal corneas, corneal tonometry may be straightforward and clinically familiar. But in modern practice, clinicians increasingly encounter eyes that do not fit the “textbook cornea” assumption on which corneal tonometry was historically built. Refractive surgery, corneal thinning, keratoconus, scarring, edema, corneal infections, scleral lens wear, keratoprosthesis, and age-related biomechanical changes can all influence the corneal surface or the way it responds to tonometry.
In those cases, a different question becomes important:
If a corneal-dependent tonometer and a corneal-independent tonometer disagree, should the corneal-independent device automatically be assumed wrong — or might the cornea itself be distorting the corneal reading?
That is the central issue this article explores.
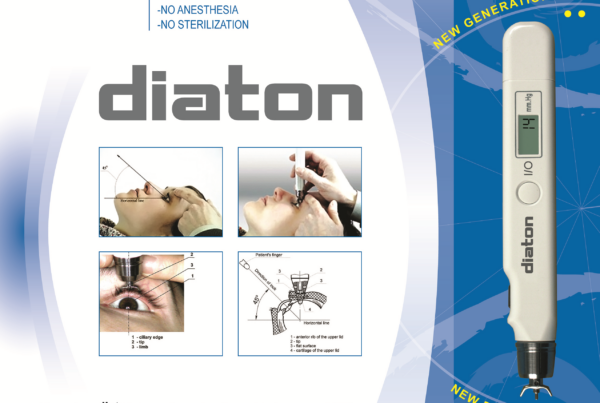
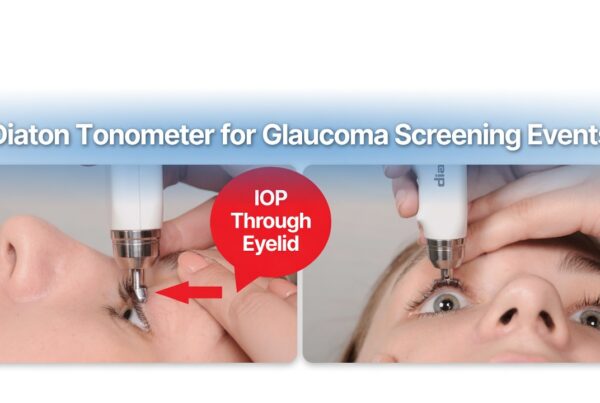
The Diaton® transpalpebral tonometer offers a different pathway for intraocular pressure (IOP) screening. Rather than measuring through the cornea, it measures through the upper eyelid over the sclera, bypassing corneal thickness, corneal rigidity, corneal hysteresis, and many of the biomechanical variables that affect corneal-based methods. In that sense, Diaton is not simply “another tonometer.” It represents a corneal-independent measurement strategy that can complement traditional tonometry, especially in patients whose corneas may no longer behave predictably.
1. Goldmann Remains Important — But the Cornea Is Not a Neutral Surface
Goldmann applanation tonometry has earned its place in ophthalmology. It is familiar, clinically embedded, and supported by decades of use. But it is important to remember what Goldmann actually measures and what assumptions it makes.
Goldmann estimates intraocular pressure by flattening a defined area of the cornea. That process is influenced not only by pressure inside the eye, but also by the physical properties of the cornea being flattened.
Among the most important variables are:
- central corneal thickness (CCT)
- corneal hysteresis
- corneal rigidity / elasticity
- post-surgical biomechanical change
- surface irregularity, scarring, or edema
- patient age and age-related corneal changes
In other words, Goldmann does not measure pressure in a vacuum. It measures pressure through a tissue layer whose properties may themselves vary substantially from patient to patient.
That does not invalidate Goldmann. It does mean that clinicians should be cautious about treating it as a perfectly neutral truth source in eyes with altered corneas.
2. The Real-World Scale of the Problem Is Much Larger Than Most Discussions Acknowledge
It is easy to think of corneal-compromised eyes as a niche problem. In reality, the population potentially affected by corneal-dependent measurement limitations is enormous.
Post-refractive surgery alone is no longer a small subgroup
More than 40 million refractive procedures such as LASIK, PRK, and SMILE have been performed worldwide, and that number continues to grow. Multiple studies have shown that corneal applanation methods may underestimate IOP after refractive surgery, because the cornea has been thinned and its biomechanics altered.
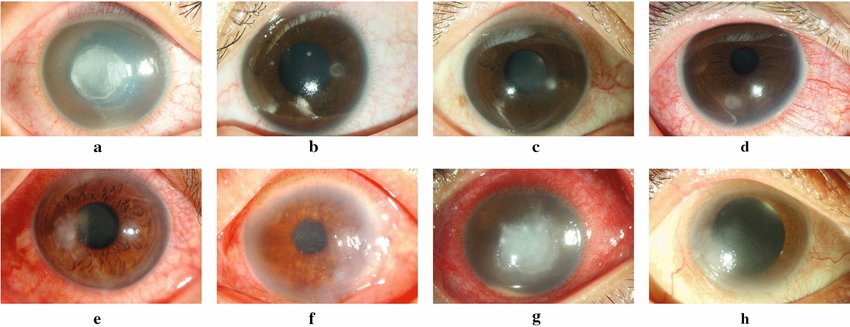
Corneal pathology is not rare
Millions of patients worldwide live with:
- keratoconus
- corneal scarring
- corneal edema
- ocular surface disease or prior infections
- post-corneal surgery changes
- Boston keratoprosthesis or other complex corneal situations
- scleral lens wear that complicates corneal-dependent assessment
Aging itself changes the cornea
Perhaps the most underappreciated issue is scale. The global population aged 40 and older is measured in billions, not millions. Corneal thickness and corneal biomechanics change with age. Natural thinning, reduced hysteresis, and age-related structural change can all influence the way corneal tonometers behave over time.
That does not mean every person over 40 automatically has a clinically misleading Goldmann reading. It does mean the population in whom corneal-dependent tonometry may be influenced by corneal variables is far larger than often appreciated — potentially hundreds of millions of patients worldwide, and broader still if one considers the sheer number of aging corneas that no longer behave like youthful “normal” tissue.
This is why corneal-independent IOP assessment should not be treated as a fringe concept. It is increasingly relevant to mainstream glaucoma care.
3. Most Tonometers Share the Same Fundamental Weakness: They Depend on the Cornea
Goldmann is not alone in this respect. Many commonly used alternatives still depend on corneal interaction to varying degrees, including:
- non-contact air-puff tonometers
- rebound tonometry (iCare)
- Tono-Pen
- other corneal applanation or indentation methods
These devices may differ in convenience, workflow, or algorithmic compensation, but most still inherit the same core vulnerability: the cornea remains part of the measurement pathway.
That means they can all be influenced — in different ways and to different extents — by:
- corneal thickness
- corneal hysteresis
- post-LASIK / post-PRK / post-SMILE changes
- keratoconus
- corneal edema
- scarring
- irregularity
- aging-related biomechanical change
This is an important point when interpreting studies that compare Diaton to Goldmann or other corneal devices. If the “reference” device is itself influenced by the cornea, then disagreement does not automatically prove that Diaton is inaccurate. It may simply mean the two devices are responding to different anatomical pathways, one of which is vulnerable to corneal distortion.
4. A Different Measurement Pathway: Through the Eyelid, Over the Sclera
The Diaton® transpalpebral tonometer takes a different approach. Instead of flattening the cornea, it measures through the upper eyelid over the sclera, bypassing corneal tissue altogether.
That distinction matters because it removes from the measurement pathway the very factors that often complicate corneal tonometry:
- central corneal thickness
- corneal hysteresis
- post-refractive surgery changes
- corneal scarring
- edema
- surface irregularity
- corneal lens-related distortion
This does not mean Diaton should replace Goldmann in every case. It does mean that Diaton can provide an independent IOP perspective that is not being filtered through the cornea.
In patients with altered corneal biomechanics, that independent perspective may be clinically valuable.
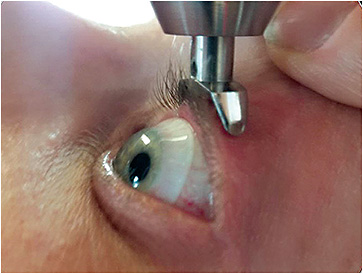
5. The Diaton Measurement Principle: Fixed Mechanics Rather Than Corneal Flattening

Diaton uses a ballistic transpalpebral measurement principle based on classical mechanics.
A small internal rod, often referred to as the floater, performs a short, controlled free-fall inside the instrument, contacts the eyelid overlying the sclera, and rebounds. The device evaluates the deceleration and rebound characteristics of that interaction.
Unlike Goldmann, it is not inferring pressure by flattening corneal tissue. Instead, it is evaluating the response of the eyelid/scleral interface to a controlled mechanical event.
Three elements of the system are fixed by design:
1. Fixed floater mass
The internal rod is manufactured to a precise weight specification.
2. Fixed drop distance
The path through which the floater travels is mechanically defined and calibrated during production.
3. Gravity-driven movement
The system depends on a controlled vertical free-fall when positioned properly.
Because these inputs are fixed, the device’s internal measurement engine is mechanically consistent by design. In practice, when readings vary, the reason is more likely to be found in positioning, tissue contact, lid handling, or patient factors than in the basic measurement engine itself.
6. Why Technique Still Matters — But Not for the Reason Critics Sometimes Suggest
A common criticism of Diaton is that it may be “operator dependent.” That criticism needs context.
The truth is that all tonometry is operator dependent to some degree. Goldmann requires proper fluorescein interpretation, alignment, applanation endpoint recognition, slit-lamp positioning, and examiner judgment. Tonopen, iCare, and air-puff systems also require technique, positioning, and patient cooperation.
Diaton has its own technique logic because it uses a different anatomical route and a gravity-driven mechanism. That does not make it unusually fragile. It simply means the operator must understand where the device is intended to measure and how to position the patient correctly.
The most important technique principles are:
Verticality
The device should be held at a true 90° vertical position. The Diaton helps the user by emitting a beep until correct verticality is reached.
Horizontal head positioning
Because the device relies on a gravity-driven free-fall, the patient’s head should be as horizontal as possible, either supine or reclined with the chin elevated.
Correct anatomical target
The upper eyelid should be lifted gently so the device lands over the tarsal plate and sclera, not over the cornea.
When those steps are followed, the device is evaluating the tissue it was designed to evaluate.
7. Predictable Causes of Higher or Lower Readings
One of the useful aspects of Diaton technique is that when technique affects the reading, the direction of that effect is often predictable.
If the lid is pulled too tightly
Excessive lid tension can make the tissue firmer and may produce a higher reading.
If the device drifts onto the cornea
The reading may become lower, because the cornea is a softer tissue surface than the intended scleral target.
This matters because it reframes technique not as “random error,” but as an understandable interaction between the device and the tissue being measured. Once the user understands the anatomical target, technique becomes more intuitive and reproducible.
8. When Tonometers Disagree, the Right Question Is Not “Which Brand Won?”
If Diaton and Goldmann produce different numbers, it is tempting to ask which device is “correct.” That is often the wrong question.
A more useful question is:
What tissues did each device measure through, and what factors may have influenced those tissues?
Goldmann measures through the cornea. Diaton measures through the eyelid over the sclera. If the cornea has been thinned by LASIK, distorted by keratoconus, stiffened by scarring, softened by edema, or altered by age, then the corneal reading itself may be the value under distortion.
This does not automatically make the Diaton number “right” and the Goldmann number “wrong.” It does mean that disagreement must be interpreted in clinical context, not by assuming that the corneal device is infallible.
That context should include:
- corneal history
- refractive surgery history
- current corneal status
- optic nerve findings
- visual fields
- imaging
- technique quality
- patient cooperation and positioning
This is the most responsible way to think about tonometry disagreement.
9. Where Diaton Can Add Particular Clinical Value
Corneal-independent IOP measurement is especially relevant in:
- post-LASIK, post-PRK, and post-SMILE eyes
- thin corneas
- keratoconus
- corneal scars or edema
- corneal infections or surface distortion
- post-corneal surgery eyes
- keratoprosthesis patients
- scleral lens wearers
- patients highly sensitive to corneal contact
It is also useful in settings where a portable, technician-friendly workflow matters:
- ophthalmology and optometry clinics
- glaucoma screening programs
- emergency departments
- urgent care
- hospital-based screening
- mobile outreach and public health settings
10. Why Diaton Also Fits Modern Workflow Needs
The clinical discussion matters, but so does workflow.
Diaton offers several practical advantages in busy clinical environments:
- no corneal contact
- no anesthetic drops
- no disposable tips or covers
- portable handheld design
- straightforward onboarding for trained staff
- helpful device feedback for verticality and reading consistency
This makes it particularly useful for ophthalmic technicians, screening programs, and clinics looking to expand glaucoma detection without adding unnecessary workflow friction.
11. A More Responsible Clinical Model: Complementary, Not Combative
The most productive way to position Diaton is not as an attack on Goldmann. Goldmann remains a foundational tool. The better clinical model is:
- Goldmann is useful in many patients with relatively normal corneas.
- Diaton offers a corneal-independent IOP perspective when corneal-dependent methods may be influenced by the cornea itself.
- If readings differ, the answer is not to assume one brand “failed,” but to interpret the discrepancy in light of anatomy, biomechanics, technique, and the broader glaucoma workup.
This is especially important as the global population ages and as the number of post-refractive patients continues to rise.
Conclusion
Goldmann applanation tonometry remains a useful and historically important method in glaucoma care. But it is not immune to the cornea. Its readings, like those of many other tonometers, are influenced by the thickness, rigidity, hysteresis, and structural integrity of the corneal tissue through which it measures.
That limitation matters on a much larger scale than many clinicians or marketers acknowledge. With tens of millions of post-refractive surgery patients, millions more living with corneal pathology, and billions of adults moving through age-related corneal change, the number of people whose IOP may be influenced by corneal variables is substantial.
The Diaton® transpalpebral tonometer offers one practical answer to that challenge. By measuring through the upper eyelid over the sclera, it removes the cornea from the equation and provides a corneal-independent screening pathway that can complement traditional tonometry.
It should not be viewed as a rejection of Goldmann. It should be viewed as an increasingly relevant tool for a world in which the cornea itself is often the variable.
Frequently Asked Questions
Why can Goldmann tonometry be inaccurate in some patients?
Goldmann applanation tonometry measures through the cornea, so its readings can be influenced by central corneal thickness, corneal hysteresis, post-refractive surgery changes, keratoconus, scarring, edema, and other biomechanical factors. In altered corneas, the measured value may reflect both intraocular pressure and corneal behavior.
Does a different Diaton reading automatically mean Diaton is wrong?
No. If Diaton and Goldmann differ, it does not automatically mean the corneal-independent device is inaccurate. The two instruments measure through different anatomical pathways. In eyes with altered corneal biomechanics, the corneal reading itself may be influenced by the cornea.
What makes Diaton corneal-independent?
Diaton measures through the upper eyelid over the sclera rather than through the cornea. This bypasses corneal thickness, corneal rigidity, corneal hysteresis, post-surgical corneal changes, and many other variables that affect corneal-dependent tonometry.
In which patients is corneal-independent IOP measurement especially useful?
Corneal-independent IOP assessment can be especially valuable in post-LASIK, post-PRK, or post-SMILE patients, in keratoconus, in eyes with corneal scars or edema, in scleral lens wearers, and in other cases where corneal biomechanics may distort corneal tonometry.
Can Diaton be used by ophthalmic technicians?
Yes. With proper training and technique, Diaton can be integrated into technician-driven glaucoma screening workflows. Its portability, lack of corneal contact, and absence of anesthetic drops or disposable tips can make it practical in busy clinics and screening programs.
Should Diaton replace Goldmann?
Diaton is best understood as a complementary tool rather than a universal replacement. Goldmann remains foundational in glaucoma care, but corneal-independent tonometry can add valuable information in patients whose corneal properties may distort corneal-based readings and is suitable for rapid glaucoma screening without drops or contact with the cornea.
Learn more about Diaton Tonometer:
- Diaton product page
- 100 Questions and Answers on Diaton
- How to use the Diaton Tonometer technique
- Diaton in post-LASIK / corneal pathology
- Diaton in emergency medicine / broader screening environments
- Glaucoma screening / glaucoma awareness
Learn more about – www.TonometerDiaton.com
Contact Team Diaton via Phone: 1-877-342-8667
Editor’s Note:
This article is intended for educational purposes for eye care professionals and healthcare providers interested in tonometry, glaucoma screening, and corneal-independent approaches to intraocular pressure assessment.